Revisiting Rebasing
Water cooler talk in the homecare industry has recently centered on the payment of 2014 claims, and the real-time effects of this year’s Case-Mix Rebasing on reimbursement levels. Most Home Health Providers crossed their fingers and hoped for the best in light of the 2014 PPS Final Rule Update and the installation of the Cost-Based Rebasing that had been anticipated for so long. Previously addressed in the HHSM Newsletter (A Response to Rebasing – 1/2/14), Rebasing was expected to redefine Home Health in terms of services delivered versus financial value, as the gradual Case-Mix creep had led to a national Case-Mix average of greater than 1.30 versus a PPS-proposed level of 1.0 for a standard homecare episode. Most well-meaning Home Health Providers, accustomed to making their homecare episodes work without assertive attention to the Case-Mix rating specifics, or the related utilization defined by that rating, proceeded down their traditional care path with the best of intentions.
Now six months into 2014, confronted with the stark reality that their traditional Case-Mix value expectations no longer apply, Home Health Providers are vocal about the effects of Rebasing. In our consulting practice, we hear from Providers who are struggling to get their bearings under the new Rebased Case-Mix levels. The commentary often heard is along the lines of “I’m shocked by what the payments are”, or “What is Medicare doing to us?”, and “We can’t make it financially if we can’t pay our bills” in response to payments with double-digit reductions. Inquiries along the lines of “What do we do and how do we fix this?” reflect Providers who are shocked, lost, or horrified (their words). List serve chatter mirrors these concerns; generally expressing a level of exasperation and frustration with the latest billing returns. This appears the latest in a long line of financial challenges for Home Health Providers, already burdened by PPS Rule benefit and programming changes that indirectly affect the bottom line.
The concerns are long-term in nature; today’s Rebasing experiences are only the latest installment in what will be shape-changing reforms for Home Health over the next decade. Most initial reactions to the real-time effects of Rebasing come from the victimization angle; “Why us, Why this, and Why now?’ Little if any of the comments are focused on an examination of internal issues that can affect Case-Mix results, such as OASIS accuracy, lack of Utilization Review (UR), billing timeliness and efficiency controls, or silo activities that compromise outcomes in this area. And even less attention is directed towards the other under-lying issues that actually define the level of outcomes on both clinical, financial, and Case-Mix levels. That includes the current element of clinician-led care programming, void of the type of UR/Clinical control seen outside of Home Health, which exists today in the homecare world.
Practical and effective solutions to the Rebasing challenges can be found in the basic philosophies behind CMS care production and delivery that applies to all Medicare Providers. Care delivery is based on a PPS-mandated acuity model, designed to effectively respond to beneficiary clinical needs, and spread out over a care continuum of individual Providers, each with a specific mode of service specialty. In the era of reform where Home Health currently finds itself, it is important to remember that CMS needs to provide levels of payment that exceed cost levels in order to retain the number of Providers required for that patient population; each Provider-type must remain healthy and viable in business terms in order to service Medicare’s population needs. The reality is that Providers unable to post positive, after-cost profit margins are soon to be ex-Providers; unable to stay in business due to the red ink in their budget sheets. So when payment reductions or programming reforms occur and the eventual result alters the fiscal payments Providers are accustomed to receiving, there is always a clinical solution that creates qualified care based on cost levels CMS expects. Seeking and finding these solutions are paramount for Home Health Providers looking to survive the reforms and continue their care mission in the future.
Progressive solutions can be found that address the current and future programming needs that Home Health Providers face. Refining the basic intrinsics of quality healthcare are the first step on the path to improved homecare performance. Stepping away from the day-to-day Home Health protocols, in a back to basics manner, helps to contrast current homecare practices and protocols against those seen across the rest of the care continuum. Focusing on the elements that affect Case-Mix performance, directly or indirectly, isolates a list of areas that becomes a roadmap for reinvention:
- Intake
- OASIS Accuracy
- SOC Utilization Review Control
- 30-day POC orders
- UR-defined Care Volumes – RN/PT/OT
- Safety-Based Frequencies
- Scheduling/Productivity
- In-Episode Clinical Control
This list references the items that define Home Health care production, and ultimately the tenor of the patient episode. Agencies who manage these essential elements of care production find themselves on the identical road as other Medicare Providers, including acute care hospitals, IRFs, and SNFs. Ironically, these are the same groups that will collaborate with Home Health in the episodic programs of the future, where we will share episodes, patients, and payments with non-homecare Providers. It seems unlikely that these Providers, all delivering UR-managed care, clinical schedules and program volumes, would interface well with a Home Health industry lacking the same quality-control elements.
HHSM SURCH Rebasing Results
UR-based care Production addresses the concerns described above as it returns total clinical control to the Home Health Provider seeking to elevate their care programs. Working with homecare Providers across the country, HHSM has installed their UR program developed for the Home Health Provider, S.U.R.C.H. – Service Utilization Review for Care in the Home. By rewiring all elements of care production described above, the referenced Providers reinvented their clinical programs with an eye on PPS compliance and efficiency. They were willing to look inwards to re-examine aspects of their current processes, seeking opportunities for gains based on quality controls, UR-managed programming and patient-centered care. The resultant improvement in their Case-Mix, clinical outcomes, and actual episode control underscores their commitment to progressive, contemporary, quality programming.
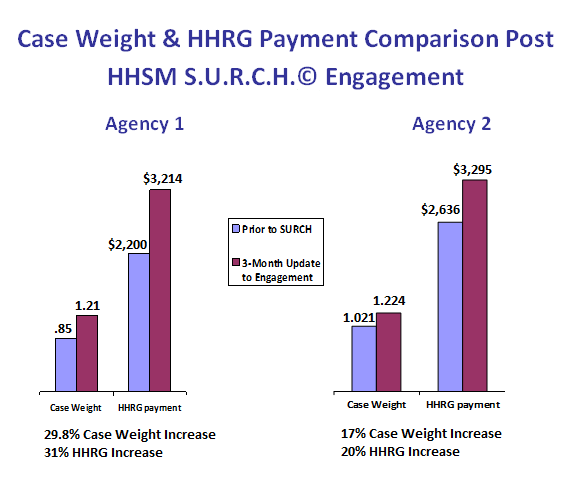
The graphs above demonstrate the level of improvement produced through use of the S.U.R.C.H. in as little as 90 days; the result of a focused effort on the part of the Home Health Providers involved. Focusing on the care production elements of a Home Health episode, they proceeded to review and assure SOC documentation for OASIS accuracy, collaborate with clinical staff for contemporary programming and care volumes, and install safety-based clinical frequencies to reduce hospital readmissions; all the while improving Case-Mix/HHRG results by double-digits. These improvements are evident and meaningful; the agencies involved enriched their Case-Mix by an average of 23.4%. As a result, they effectively neutralized the impact of 2014 Rebasing while simultaneously improving the level of qualified, PPS-compliant, audit-proof care produced and delivered. In addition, all of these changes were achieved over a 3-month duration.
The effects of this process cannot be overstated. Agencies who were operating at a financial loss prior to Rebasing found their losses increasing in their 2014 claims as the Rebasing further impacted their negative margins. As mentioned above, most Providers in this situation place the blame solely on Medicare, discounting the changes that OASIS accuracy, Utilization management, and quality care service delivery can produce. For Providers who find themselves in this situation, the future offers even greater challenges. Projections of greater than 50% of Home Health Providers posting negative margins are common, and some states will have 100% Providers posing negative margins by today’s standards. The standard response is to lobby to repeal the Rebasing reductions; this seems unlikely to occur due to the consistent approach Medicare has employed combined with the desire to standardize care processes across the care continuum.
So the options are clear and becoming clearer with each new level of reform or payment reduction. The predominant issue is whether or not a particular agency can find the will to evolve their care processes and staff to the level of care requirements the future will pose. Some Providers will adapt to continue on their care path into the future. Other Providers will choose not to rewire care and will attempt to retain their viable business status as long as possible. But many Home Health Providers will continue un-informed of the processes and care modifications that will usher them into the ACO era. By doing so, they will have inadvertently chosen to allow their clinicians to dictate the closure of their agency.
HHSM readers can receive a free 5-case S.U.R.C.H. assessment to assess their current status regarding Case-Mix and other elements related to the statistics above. Contact HHSM at 1-866-449-HHSM or at www.homehealthstrategicmanagement.com
Arnie Cisneros, P.T., President of Home Health Strategic Management, is the most progressive speaker in homecare today. He provides coaching and consulting services to providers on a national basis regarding S.U.R.C.H. and other clinical management protocols for quality outcomes.